Abstract
Background
The United Arab Emirates had approved the COVID-19 vaccine for children. Assessing parents’ acceptance of the vaccine for their children will influence decision-making in the COVID-19 vaccine roll-out.
Method
Parents registered in the Abu Dhabi Department of Education (12,000 families) were invited to complete an online questionnaire from 8th September 2021 to 17th October 2021. Out of the 12,000 families, 2510 (21%) participants answered the survey. The questionnaire investigated the parents’ attitudes and beliefs regarding the COVID-19 vaccine.
Results
The vaccination rate among this group of respondents was high, with 2255 (89.9%) having received two doses and 1002 (45.5%) having already received a booster dose. Acceptance of the respondents to vaccinate their children was high, (75.1%) said they would vaccinate their children, with 64.4% reporting that they would immediately vaccinate their children if the vaccine were made available. Determinants of COVID-19 child vaccination acceptance included the respondent’s vaccination status—i.e., if the respondent is already vaccinated (OR 4.96 [2.89–8.53]) or has taken the third dose (OR 2.37 [1.4–4.01])—their children’s age (OR 1.11 [1.30–1.18] for older children), and their trust in the following information sources: the government (OR 2.53 [1.61–3.98]), health care providers (OR 1.98 [1.2–3.24]), or social media (OR 2.17 [1.22–3.88]). Increased level of education had a negative impact on the acceptance of giving the vaccine to children (OR 0.63 [0.52–0.77]); fear of side effects OR 0.000164 (0.000039–0.001) was another determinant. The main factor that encouraged parents to give their children the vaccine was to protect their child’s health as reported by 1537 (55.5%) participants.
Conclusion
The Abu Dhabi community is highly accepting of the vaccine for their children. Future studies of how this vaccine acceptance can influence the pandemic are needed.
1. Introduction
The global COVID-19 vaccination rate was 50% by November 2021. The United Arab Emirates (UAE) is leading the global vaccination program with 98% of its adult population having received one dose, and 88% being fully vaccinated. By October 2021, 40% of Abu Dhabi Emirate children, 3–17 years, were fully vaccinated against COVID-19. In the UAE, the Pfizer COVID-19 vaccination was approved for children aged between 12 and 15 years in May 2021. Sinopharm COVID-19 vaccine safety study on children was started in Abu Dhabi in June 2021, and shortly after, in August 2021, the Sinopharm COVID-19 vaccine was approved for emergency use for children aged three years and older. The high vaccination rate of the UAE population is facilitated by the UAE government’s efforts to support the vaccination program. Vaccine acceptance among the UAE population was reported to be among the best in the world.
Vaccinating children against COVID-19 is a difficult debate. With the limited supply of vaccines, children may not be considered a priority group for the vaccine. There is also the fact that the safety of the vaccine for children is still an evolving knowledge, with early trial results hinting that those vaccines could be safe for children. However, a review by Kostoff suggests that the risk of death from COVID-19 decreases drastically as age decreases, and the long-term effects of the vaccination on lower age groups will increase their risk–benefit ratio. Later studies have been focused mainly on mRNA vaccine trials as most vaccines rolled out are of this type. Countries worldwide are increasingly introducing the COVID-19 vaccine to children and how the pandemic progresses will determine their roll-out among children globally.
Children represent a significant source of COVID-19 infection for adults at higher risk. Even with full vaccination, the risk of infection, although reduced substantially by 5.8 times, will not be completely eradicated [11]. Children are a large proportion of the population; in the UAE, those younger than 15 years old constitute 14.7% of the total population, and therefore, being a source of infection, especially with school re-opening, children carrying COVID-19 virus will pose a risk to any pandemic mitigation efforts.
Abu Dhabi is the largest Emirate in the UAE and the capital city of the UAE. Abu Dhabi, and the UAE in general, has handled the COVID-19 pandemic well, with the best resources and strategies. This was seen from the early stages and in all aspects, such as healthcare capacity and non-pharmacological and pharmacological interventions accessibility. For example, COVID-19 testing and adult COVID-19 vaccination were accepted well by the UAE population, and this was reflected in the high acceptance rates reported, compared to other countries in the world, as well as a comparatively lower mortality rate.
Children’s COVID-19 vaccine was introduced in 2021, with the Sinopharm vaccine being introduced to the Abu Dhabi population in November 2020, while Pfizer was introduced early in 2021. At the start of the children’s vaccination program, 40% of Abu Dhabi children were fully vaccinated by the end of October, and in some Abu Dhabi schools, more than 50% vaccination rates among their students were seen and above 95% among teachers by November 2021. The vaccination was rolled out in community sites, in specially built vaccination centers, and in all ambulatory healthcare services and primary care centers, which ensured accessibility for all families. During the pandemic, the government provided weekly updates through the media to inform the public of all information related to the COVID-19 surge and vaccination uptake and importance.
The vaccination centers followed the directive of the Abu Dhabi Department of Health (DOH), which had a surveillance system for the COVID-19 vaccination campaign to monitor any possible adverse events. This was made possible as Abu Dhabi Healthcare system had Electronic Medical Records implemented across all healthcare facilities. As well, email communication to all facilities were established to update them about guidelines and requirements such as reporting vaccine adverse events.
Parents’ acceptance of the COVID-19 vaccine for children varied globally, with 89% in China to very low rates in Europe. Assessing the acceptability of the COVID-19 vaccine for children is critical to probe the parents’ intentions and facilitate better strategies in the COVID-19 vaccine roll-out and minimize unnecessary delays. This study evaluates the acceptance of children’s COVID-19 vaccine by the parents of school students in Abu Dhabi, UAE.
2. Method
This is a cross-sectional questionnaire-based study targeting parents registered in the Abu Dhabi education department database. Abu Dhabi is the capital of the UAE with a population of nearly 1.5 million. Government school students from primary to secondary grade (aged 3–20) were included in this study. Private schools were not included as they had a different database. A total of 12,000 families were sent an online survey, both in Arabic and English, through https://www.surveymonkey.com. No exclusions were applied, and all nationalities living in the UAE were included. Parental consent was required to complete the survey. Information about the study was included on the first page of the survey for self-completion if the subject consented to participate. Data was collected from 8th September 2021 to 17th October 2021. This period coincided with the roll-out of Sinopharm children vaccination for all children aged 3 years and older. As this was a coincidence, the survey did not include the vaccination status of the children but only studied the parents’ intentions.
The questionnaire used a modified version from a few studies on similar topics that were published recently due to the lack of a well-validated questionnaire in this area. The resulting questionnaire was reviewed by an expert panel of eight people from school health, public health, and family medicine specialties for face validity.
The survey comprises three sections. Section one is concerned with parents’ demographics, such as age, sex, nationality, marital status, educational level, occupation, pregnancy status, as well as their history of COVID-19 infection, their vaccination status, and their possible experience of the loss of a loved one or other non-COVID-19 related health problems. Section two discusses their children, how many are they, their ages, health status, and if the parents wish to vaccinate their children. Additionally, it includes questions on attitudes regarding the COVID-19 vaccine, such as worries and rationales for vaccinating their children. Section three includes public trust and general vaccine attitude questions. Questions were dichotomous yes/no and multiple-choice questions. Responses to multiple-choice questions measured agreement with 5-point Likert scales.
Of the 12,000 registered families in the database, 2771 (23.1%) consented to participate. Another 261 did not answer any questions, leaving 2510 (21%) participants who answered the survey.
2.1. Statistical approach and power calculations
Analysis was done using the SPSS program version 28. Frequencies and cross-tabulation were used to describe the population. Regression analysis was used to identify significant interactions and predictors of vaccine acceptance. A p-value of <0.05 was considered significant.
2.2. Ethical consideration
Abu Dhabi COVID-19 Research Ethics National Committee approved the study (approval number: DOH/CVDC/2021/1150).
3. Results
Parents participating in this study responded favorably to the question, “If COVID-19 vaccine was available, will you vaccinate your children?” Three-quarters of them (75.1%) agreed to vaccinate while one-quarter were hesitant. Concerning the timing of the vaccine, (64.4%) of respondents reported that they would immediately vaccinate their children, 5.6% have already done it as part of the vaccination trial (phase III), 13.2% will wait for some people to vaccinate their children first before deciding, and 9.7% will wait for the majority of people to vaccinate their children, while 7.1% were still unsure. Unsurprisingly, (59.1%) of those intending to vaccinate their children support the suggestion that children should require COVID-19 vaccination to physically attend school, (35.3%) strongly agreed, and (23.8%) agreed.
Table 1 describes the participants’ demographics and Table 2 reports factors that may influence vaccine acceptance for children and parents. Of the respondents who didn’t take the vaccine, factors related to disfavor were: fear of vaccine-related side effects in 30.1% (1 2 2) of respondents and 22.5% (91) were from the exempted group from taking the vaccine. A similar figure of 17.5% (71) and 16% (65) reported a lack of enough and reliable data on the vaccine and did not believe that the vaccine works, respectively. A minority of 13.8% (56) reported a lack of trust in the vaccine manufacturers. Similarly, the main reason for not vaccinating children is fear of side effects 82.5% (4 7 0), followed by a lack of reliable and enough data on COVID-19 vaccines 53% (3 0 2).
Table 1. Participants characteristics.
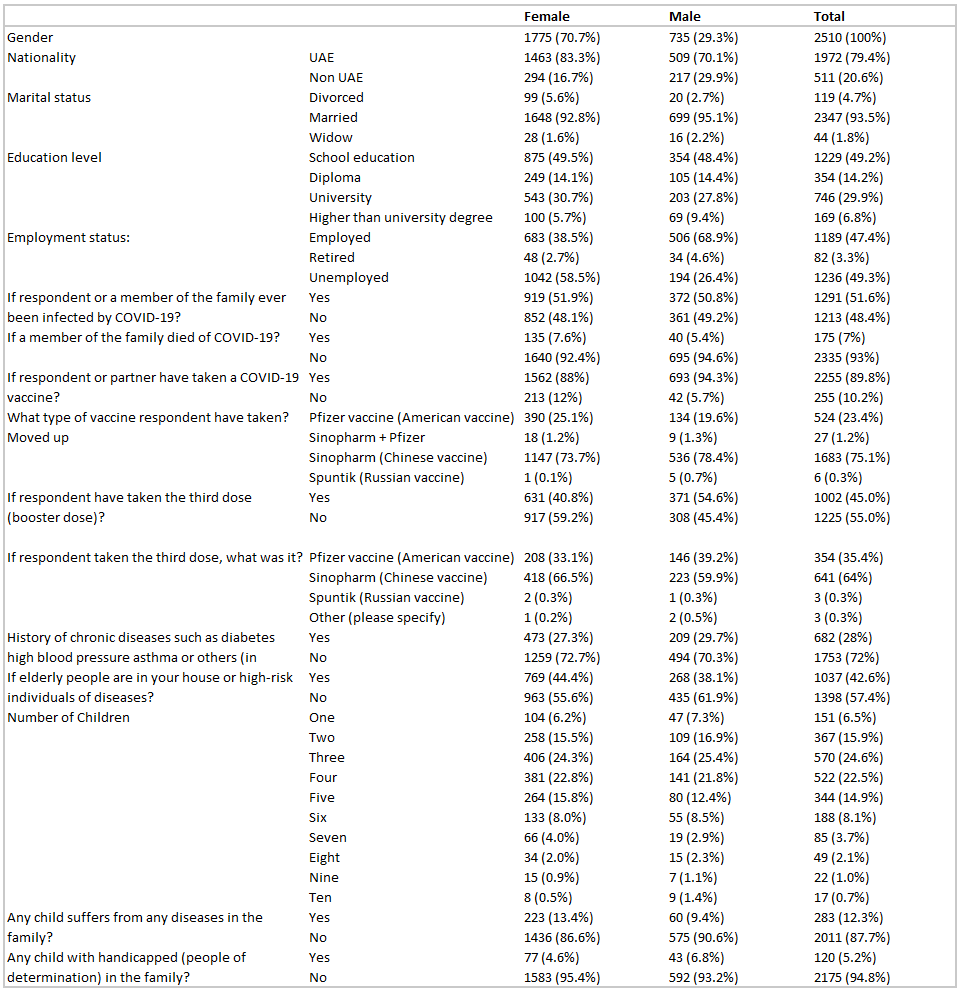
Table 2. Factors that may influence vaccine acceptance for children and parents.
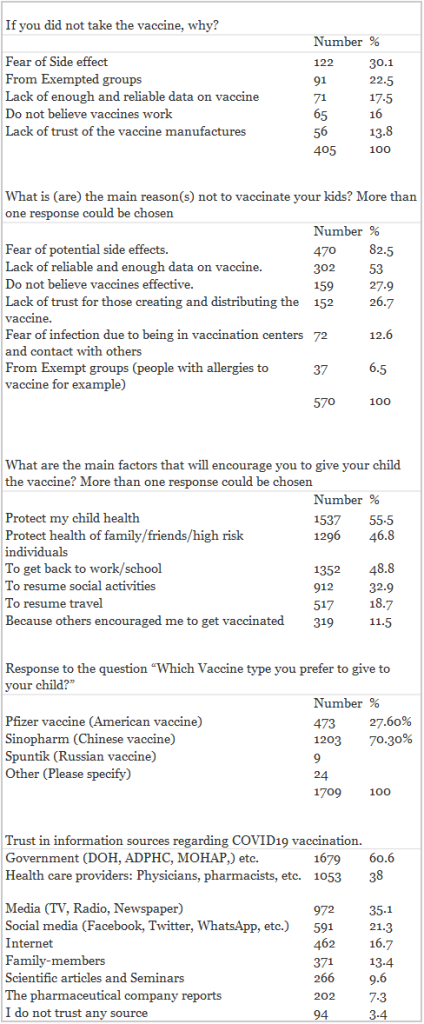
On the other hand, the main factors that encouraged parents to give their children were to protect the child’s health reported by 1537 (55.5%), to protect the health of the family, friends, or high-risk individuals 1296 (46.8%), to get back to normal life activities including going back to work/school (1352, 48.8%), resume social activities (912, 32.9%), and to be able to travel (517, 18.7%). 319 (11.5%) reported that it could be because of the encouragement of others to get the vaccine. Most respondents preferred choosing Sinopharm vaccine 1203 (70.3%), followed by Pfizer vaccine 473 (27.6%) for their children.
With regard to a trustworthy source of information about COVID-19 vaccination (Table 2), 1679 (60.6%) of the participants answered government-related sources, followed by health care providers 1053 (38%) and media, such as television, radio, newspaper 972 (35.1%). Although only 591 (21.3%) considered social media a trusted source of information, 72.4% agreed that it influences parents’ decision to vaccinate.
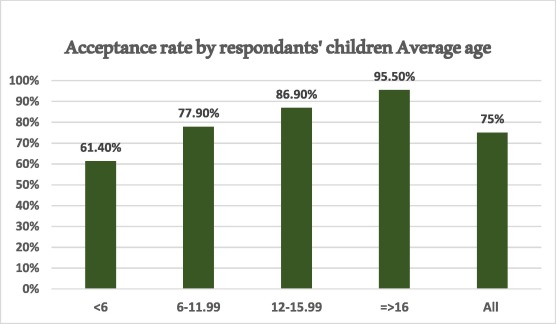
Determinants of COVID-19 vaccine acceptance are shown in Table 3. Better acceptance was found related to the vaccination status of the respondents. More acceptance was seen among those being vaccinated OR 4.96 (2.89–8.53) or had taken the third dose OR 2.37 (1.4–4.01). Parents are more likely to accept the vaccine if the children are older OR 1.11 (1.30–1.18) (Fig. 1). This is made evident through the vaccine acceptance rates among the parents of children in different age groups. Parents of children >15 years old have the highest acceptance (95.5%). While the rate of acceptance is (86.9%) among parents of children in the age groups 12–15 years, (77.9%) among 6–11 years old children’s parents, and (61.4%) in <6-years-olds’ parents (Fig. 1). Fear of side effects seem to play a role and was associated with less acceptance, OR 0.000164 (0.000039–0.001).
Table 3. Determinants of parents’ vaccine acceptance for their children.
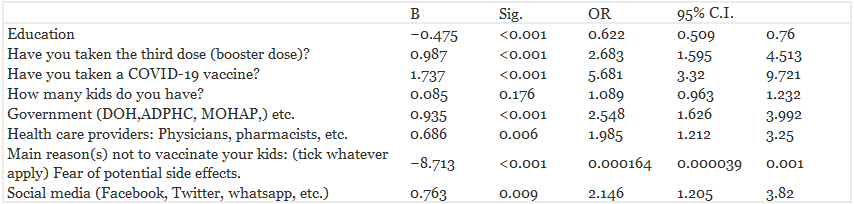
Fig. 1. Acceptance rate of COVID-19 vaccine by the respondents’ children’s ages mean.
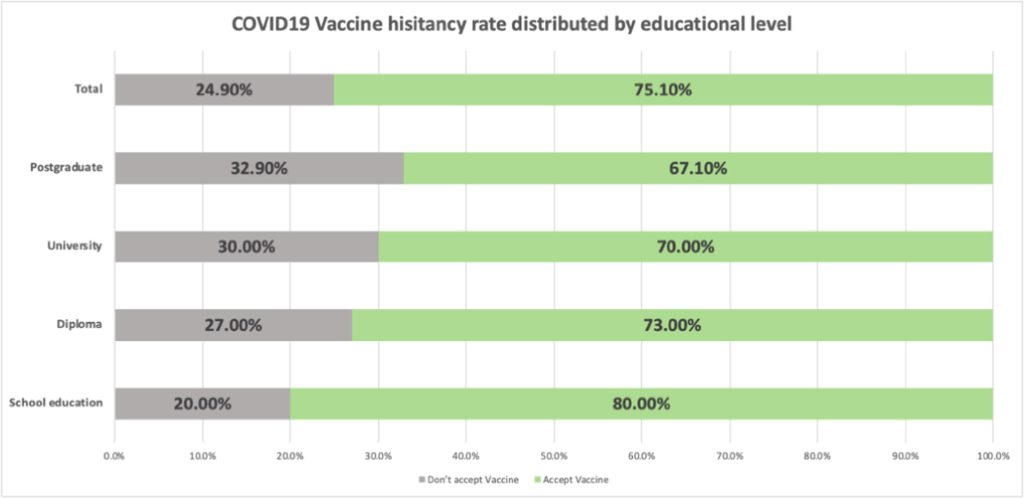
An important determinant was the trust in information sources with more trust in government sources, OR 2.53 (1.61–3.98), health care providers, OR 1.98 (1.2–3.24), and social media OR 2.17 (1.22–3.88). Unexpectedly, having a higher level of education had a negative impact on the acceptance of giving the vaccine to children OR 0.63 (0.52–0.77).
Fig. 2. COVID-19 vaccine hesitancy rate distributed by educational level.
All other variables, such as parents’ gender, marital status, employment, number of children, chronic diseases in the child or family or presence of elderly in the family, history of COVID-19 infection in self or family member or death related to COVID-19 infection all were not determinant of the decision to vaccinate.
An additional analysis of the determinants of parents’ vaccination status showed that it was more likely that participants is vaccinated if they were males, employed, had fewer children, older children, and agreed less with the statement “do not believe the vaccine is effective”. As well the COVID-19 vaccinated parents were more accepting to vaccine their children, wanted to resume social activities, had COVID-19 or a member of their family had been infected by COVID-19 and agreed that children required vaccination to rejoin schools physically, and trusted the government more. Similarly, participants were more likely to take the third dose if they were males, employed, had fewer children, older children, agreed less with the statement “do not believe vaccines effective,” more accepting of the vaccine for their children, wanted to resume social activities, wanted to get back to work/school, had COVID-19 or a member of their family had been infected by COVID-19, and agreed that children required vaccination to rejoin schools physically, and are from Al Ain city.
4. Discussion
Abu Dhabi’s adult population is nearly 90% vaccinated at the time of this study data collection. This study indicates that parents of school children in Abu Dhabi have high acceptance of the COVID-19 vaccine for their children. Three out of four of the 2510 participants agreed to vaccinate their children, and two out of three intend to vaccinate them immediately once it is available. This acceptance was during the launch of the Sinopharm vaccine for children aged 3–18 years and four months after approving the Pfizer vaccine for the age group 12–15 years in the UAE. By the end of October 2021, the Abu Dhabi community had fully vaccinated 40% of their children, and some Abu Dhabi schools reached more than 50% vaccination rate among their students, and above 95% among teachers in November 2021 [17]. Most of the participating parents (70%) prefer the Sinopharm vaccine.
The rate of vaccine acceptance in this group of participants is among the highest globally. However, COVID-19 vaccination acceptance rates for children varied even within the same country during different stages of the pandemic [22]. Therefore, the reported rate of vaccine acceptance reflects the rate during the period data was collected only. Possible influencing factors on the acceptance rate can be the timing of the survey during the pandemic, the surge or decline of COVID-19 cases, age group, or the government policies enforced. For example, in a study by Goldman et al., vaccine acceptance surveys were completed in phase 1 (March–May 2020) and phase 2 (December 2020–March 2021). In that study, fewer caregivers planned to vaccinate against COVID-19 in phase 2 compared to phase 1 (64.5% and 59.7%), respectively [22]. Similarly, in Saudi Arabia, the COVID-19 vaccine was accepted by half the respondents in one study and another two Saudi studies reported an acceptance rate of 28.1% and 24%. [23], [24], [25]. In a survey conducted among mothers in China, the hesitancy rate was 8% [26]. In another study in the China Northwest region, only 50.0% wished to vaccinate their children, with the age of children evidently playing a role as it was 32.7% for those with children aged 0–5 and 73.3% for those with children aged 11–18 [27]. Such variation in the age of the children was a significant determinant in this study as well. Parents tended to be protective and more hesitant if they had younger children. As side effects were the main reason for hesitancy in this study, the perceived vulnerability of the younger age group could explain the hesitancy. Another factor could be that the Pfizer vaccine in the UAE was introduced earlier for the older age group of children, and therefore, it could be already accepted as a norm in the UAE to vaccinate children aged 12 years and older. This was seen in China with children’s vaccine being approved for those aged between 15 and 18 years since July 2020, and for this age group acceptance rate was reported to be very high 89.3% [18] when compared to this study rate in the same age group (95.5%).
In Europe, Canada, and the United States, the rate of vaccine acceptance was varied. It was 29.6% in Italy [19], 60% in Portugal [28], 44% in Poland [29], 63% in Canada [30], and 49.45–69.2% in the US [31], [21]. As mentioned, this rate may fluctuate and is difficult to explain. Nevertheless, in Abu Dhabi, the possible explanations could be parents’ experience with the COVID-19 vaccine and their very high vaccination rate, in addition to their possible perception of susceptibility. Especially, since the country went through four COVID-19 pandemic waves, with the fourth extending over seven months. This can be noticed from their response that nearly half of the participants had a COVID-19 case in their family, and 7% know about a COVID-19 death in their family.
Predictors of better acceptance, in addition, were employment, lower educational level, and having older children. In Abu Dhabi, the government had placed incentives at the workplace for those vaccinated for many months before this study was conducted. Such as requiring less COVID-19 testing for the vaccinated and fewer restrictions at workplaces and public places. This might explain the increased acceptance of the vaccination among the employed since they may have experienced easier mobility and fewer restrictions while being vaccinated. It is also noteworthy that the employed group may have felt more susceptible to the virus than those who are unemployed and stay at home. This is evident from the regression analysis of determinants of vaccination for the parents, being fully vaccinated or vaccinated, with third dose participants less in agreement with the statement “do not believe vaccines effective,” trusting that vaccination is their way to resume social activities and get back to work/school. It also shows from the regression analysis that trust in government and healthcare authorities is strongly determining the population trend to accept vaccination for them and their children, more even than the healthcare professionals. This is contrary to other countries. Maintaining the trust of the public and continued reassurance was a cornerstone of the UAE government’s response during the pandemic. The leaders always stressed the willingness for unlimited support for the population’s health. Such efforts contributed to more surveillance coverage, lower mortality rate, and earlier and higher vaccine availability and rate [1], [2], [5], [6]. Trust in the government was reported by the population in several studies [4], [32], [33]. This was confirmed in a recent systematic review and meta-analysis of the acceptability of vaccination against COVID-19 and its predictors, trust in the government was a positive predictive factor of vaccination willingness in 20 surveyed countries [34], [35]. Additionally, on average, stronger and faster stringency of anti-pandemic measures and a smaller number of deaths are positively associated with trust in the governments’ handling of the pandemic [36]. Such large heterogeneity between countries in trust could be changing as well and it is worthwhile to be monitored and targeted by the government to ensure better public adherence to evidence-based health interventions.
The main reason for the Abu Dhabi community to get the COVID-19 vaccine or accept it for their children was to protect their children and families. This was similar to other counties [37], [38]. On the other hand, although fear of side effects was the main reason for the participants not to take the vaccine, with one-third admitting their fear, fear was reported more (82.5%) by hesitant participants to accept it for their children compared to (0.1%) reported by the accepting group.
There is a need to deliver precise information about the vaccine to ensure its appropriate uptake as the second reported factor for parents not taking the vaccine or not giving it to their children is the lack of reliable and enough data about the vaccine or lack of trust for those creating it and distributing the vaccine. Most respondents agree that mass media can influence parents’ decision to vaccinate their children, and therefore, mass media may have a significant role in better informing the community. Nevertheless, sources are essential, and as per this study, government officials and healthcare workers were the most trusted. There may be sources misinforming the public that need to be studied as those with higher education are more reluctant. Although, due to not controlling for age, this can be a confounder effect as many studies found the country with more acceptance among higher education [35], [38]. It is expected that knowledge about the pandemic and COVID-19 infection and COVID-19 disease risk can be more appreciated among the higher education group, which may positively influence their vaccination decision. It is noteworthy that their education level did not affect the parents’ vaccination decision for themselves. However, this can be explained by the increasing restriction on non-vaccinated people in Abu Dhabi, such as workplaces and government entities requiring vaccination.
The type of COVID-19 vaccine could be a possible factor that can influence acceptance variability in different countries. The UAE population seems to trust the Sinopharm vaccine and have a positive attitude toward it, as shown from this study and another study by Ahmed et al. [4]. The vaccine choice is with Sinopharm in the lead (75%) when compared to Pfizer (23%). This is similar to a study conducted among healthcare workers who preferred Sinopharm [13]. Most parents have taken the Sinopharm vaccine, and most of them like it for their children. The Sinopharm vaccine was introduced to the Abu Dhabi population in November 2020, while Pfizer was introduced early in 2021. Sinopharm showed acceptable effectiveness with far fewer side effects [6], and had therefore, gained more trust among this group of participants, with two-third of the participants preferring Sinopharm.
Most of the surveyed population agreed children should be vaccinated before joining schools physically. Nevertheless, almost one-quarter of them disagree. Although some countries have mandated the vaccine for older age groups of children to attend school physically, the UAE government has not necessitated it for schools or work. It represents an ethical dilemma of weighing the clear benefit of the vaccine and the relatively minimal vaccine safety issues to respecting parents’ autonomy of choosing not to vaccinate their children and be allowed to attend school physically, with the risk that an unvaccinated child in the school raises the risk for all who took the vaccine and their families.
The strength of this study is that the UAE children’s COVID-19 vaccination program is a reality for the respondents, unlike other studies that represent a different addition to this area of study. The other strengths are that the vaccine program included those aged three years and above, was conducted in all Abu Dhabi schools, and was a national survey. While limitations were missing, the age of the parent and the limitation of generalizability to different pandemic stages as parents’ willingness may change as the perception of susceptibility changes due to the decrease in COVID-19 cases and the reassurance of the high vaccination.
5. Conclusion
The milestones reached by Abu Dhabi in children’s COVID-19 vaccination can be attributed to a well-prepared and accepting population. Significant determinants were parents’ vaccination status and their trust in government and healthcare information sources, while the fear of side effects is the main identified barrier. Such determinants of vaccination acceptance can shed light on how the COVID-19 vaccination program may progress locally and internationally.